

- Advertisement -
Childhood Obesity | Causes, Risks & Prevention Guide
Childhood Obesity — Causes, Effects & Real Solutions
- Advertisement -
Childhood Obesity Causes, Consequences
Imagine walking into a pediatrician’s office and being told that your child’s weight is putting them at risk for type 2 diabetes — a disease once considered an adult problem. This is the reality for millions of families today, and it’s becoming more common by the year. Childhood obesity has evolved from a niche medical concern into one of the most serious global public health crises of our era. It doesn’t just affect how a child looks or feels today — it sets the stage for a lifetime of health challenges that are costly, painful, and often preventable.
We’re not talking about a child being a bit “chubby” or going through a phase. We’re talking about a complex, chronic disease that reshapes physiology, mental health, and life trajectory. The scale of the problem is staggering, and yet it continues to be misunderstood, stigmatized, or brushed off. This article breaks down everything you need to know about childhood obesity — the hard data, the root causes, the health fallout, and most importantly, what families, doctors, schools, and policymakers can do to reverse this trend.
What Is Childhood Obesity? Defining the Problem
Before we dive into solutions, we need to understand what we’re actually dealing with. Childhood obesity is a medical condition in which a child’s body carries excess fat to a degree that negatively affects their health. But it’s not as simple as looking at a number on a scale. The definition is nuanced, and the tools used to diagnose it are specific to age, sex, and developmental stage.
How Is Childhood Obesity Diagnosed?
The primary measurement tool used by clinicians is the Body Mass Index (BMI), which calculates the ratio of a person’s weight in kilograms to the square of their height in meters. However, for children, BMI doesn’t work exactly the same way as it does for adults. In pediatric medicine, BMI is plotted on growth charts that account for a child’s age and biological sex, producing what’s called a BMI percentile. According to the Centers for Disease Control and Prevention (CDC), a child whose BMI falls at or above the 85th percentile for their age and sex is considered overweight, while a child at or above the 95th percentile is classified as having obesity. This distinction matters because children naturally carry different amounts of body fat at different stages of development, and a single universal threshold would be misleading. If your child’s doctor raises concerns about their BMI percentile during a routine checkup, it’s not cause for panic — but it is absolutely worth taking seriously and exploring further with a healthcare professional.
The Difference Between Overweight and Obese in Children
Many parents use the terms “overweight” and “obese” interchangeably, but clinically, these represent different points on a spectrum of risk. Being overweight (85th–94th percentile BMI) is a warning signal — it means a child is trending toward obesity and that preventive action is highly advisable. Obesity (at or above the 95th percentile) represents a more serious condition where excess body fat is already present in amounts likely to impair health. There’s also a category called severe obesity, which is defined as a BMI at or above 120% of the 95th percentile — a classification that carries substantially elevated health risks and requires more intensive intervention. The World Health Organization (WHO) classifies obesity as a chronic, relapsing disease arising from complex interactions between genetics, neurobiology, eating behaviors, access to a healthy diet, market forces, and the broader environment — a definition that rightly situates the problem beyond individual willpower or parental negligence.

Childhood Obesity Statistics: The Numbers That Should Alarm Us
If you’re wondering whether childhood obesity is “really that bad,” the numbers will give you your answer quickly and unambiguously. The data from global and national health organizations in 2024 and 2025 paint a picture that is both alarming and urgent.
Global Prevalence of Childhood Obesity
Over 390 million children and adolescents aged 5 to 19 were overweight in 2022, including 160 million living with obesity. WHO Let that number sink in for a moment — 160 million children. That’s nearly half the population of the United States, and it’s just the count of children classified as obese, not merely overweight. In a landmark 2025 report, UNICEF revealed that obesity has surpassed underweight as the more prevalent form of malnutrition among school-aged children globally, affecting 1 in 10 — or 188 million — school-age children and adolescents. UNICEF This is a profound and historic shift. For decades, the global health narrative around children focused on hunger and undernutrition. Now, for the first time, obesity is the bigger numerical problem in most regions of the world.
According to projections from the World Obesity Federation, 158 million children and adolescents aged 5 to 19 were expected to experience obesity in 2020, rising to 206 million in 2025, and a projected 254 million by 2030. PubMed Central These aren’t just statistics on a page — they represent children who will grow up facing diabetes, heart disease, depression, and shortened lives unless we act. The trajectory is steep, and without large-scale interventions, global nutrition targets set for 2025 and 2030 are unlikely to be met. Research published in early 2025 confirmed that in the last 20 years, the global prevalence of childhood overweight and obesity has risen from 5.4% to 5.7%, with Asia (accounting for over 18 million affected children) and Africa (over 10 million) bearing the largest numerical burden. PubMed
Childhood Obesity in the United States
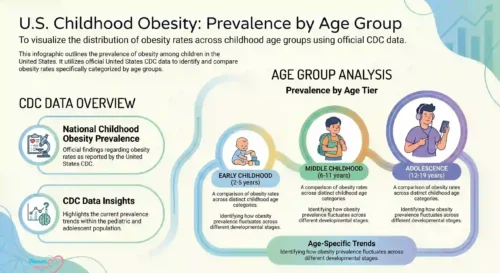
The United States is one of the hardest-hit high-income countries. From 2017 to March 2020, the prevalence of obesity among U.S. children and adolescents was 19.7%, meaning approximately 14.7 million U.S. youths aged 2 to 19 years have obesity. The prevalence climbed with age: 12.7% among children aged 2 to 5, 20.7% among those 6 to 11, and 22.2% among adolescents aged 12 to 19. CDC These numbers show a deeply troubling trend — by the time American kids reach their teens, nearly one in four has obesity.
The most recent data from the National Survey of Children’s Health (2023–2024) shows that 16.1% of youth ages 6 to 17 had obesity, with significant racial and ethnic disparities. Non-Hispanic Black children had an obesity rate of 23.0%, Hispanic children 20.6%, while Non-Hispanic White children had a rate of 12.8%, and Non-Hispanic Asian children the lowest at 9.3%. Stateofchildhoodobesity The income gap is just as stark. Obesity prevalence was 25.8% among children with family incomes at or below 130% of the Federal Poverty Level, compared to just 11.5% among those with family incomes above 350% of the FPL. CDC As Dr. David Culpepper, clinical director of LifeMD, has noted, the obesity rate being twice as high for children below the poverty line strongly suggests that access to resources gives parents a much broader range of choices regarding nutrition, and that poverty itself creates barriers to healthy eating that go far beyond personal decision-making.
| Age Group | Obesity Prevalence (US, 2017–2020) |
|---|---|
| 2–5 years | 12.7% |
| 6–11 years | 20.7% |
| 12–19 years | 22.2% |
| All ages (2–19) | 19.7% |
What Causes Childhood Obesity?
This is the question at the heart of the crisis — and it’s one that demands a nuanced answer. Childhood obesity is not caused by laziness, bad parenting, or a simple lack of discipline. It’s a multifactorial condition shaped by biology, behavior, environment, socioeconomics, and culture, all interacting in complex ways. Think of it like a river flooding — there isn’t one broken dam; there are a dozen smaller failures upstream, and each one adds to the surge.
Dietary Habits and Ultra-Processed Foods
One of the most powerful drivers of childhood obesity in the modern world is the dramatic shift in what children eat. In Mexico, sugary drinks and ultra-processed foods account for 40 percent of children’s daily calories UNICEF — and that’s far from a uniquely Mexican problem. Across the globe, children are being raised in food environments saturated with ultra-processed products: packaged snacks, fast food, sugar-sweetened beverages, and convenience meals that are engineered to be highly palatable but nutritionally hollow. These foods are energy-dense, aggressively marketed, and deliberately designed to override the body’s natural satiety signals. Children aren’t just eating more calories; they’re eating calories that do little to nourish them while driving rapid fat storage. Advertising directed at children amplifies this effect, creating preferences and brand loyalties from a very early age that are extraordinarily difficult to reverse later in life. The food industry’s profit motive and children’s cognitive vulnerability to marketing form a dangerous combination that parents and schools alone cannot counteract without systemic policy change.
Physical Inactivity and Screen Time
The decline in physical activity is the other side of the energy-imbalance equation. In developed countries, sedentary activity is commonly in the form of “screen time” — television, video games, internet, and other media. National surveys in the United States have found children between 8 and 18 years spend an average of 7.5 hours daily viewing media, while those under age 6 spend nearly two hours daily. PubMed Central This is an extraordinary amount of time spent sedentary, and its impact on caloric expenditure and metabolic health is substantial. Researchers note that something happens around ages 9 to 10 where children’s motivation to be active decreases while their motivation to be sedentary increases, and being physically active as a child gets older means shifting from unstructured play on a playground to more organized activities like sports — a shift that requires access, money, and transportation that not all families have. NIH News in Health The built environment also plays a critical role. Children in neighborhoods without safe parks, playgrounds, or bike paths are structurally disadvantaged when it comes to physical activity, regardless of how motivated their parents may be.
Genetic and Biological Factors
It would be incomplete and unfair to discuss childhood obesity without acknowledging the role of genetics and biology. Research consistently shows that children with one or both parents who have obesity are significantly more likely to develop obesity themselves — not just because of shared eating habits, but because of genuinely inherited genetic predispositions affecting metabolism, fat storage, appetite regulation, and hormonal signaling. Certain gene variants affect how efficiently the body processes calories, how quickly it triggers feelings of fullness, and how it responds to physical activity. The varied nature of obesity includes genetic, environmental, and lifestyle factors, and its causes are deeply rooted in complex biological mechanisms that are not fully within any individual’s control. PubMed Central Some children also develop obesity as a side effect of medications like corticosteroids or antipsychotics, or as a consequence of underlying medical conditions such as hypothyroidism, Cushing’s syndrome, or Prader-Willi syndrome. These cases are less common but critically important to identify, as the treatment path is very different.
Socioeconomic and Environmental Influences
Perhaps the most underappreciated driver of childhood obesity is socioeconomic inequality. Low-income families face a constellation of structural barriers that make healthy living genuinely harder: food deserts where fresh produce is scarce and expensive, unsafe neighborhoods that limit outdoor play, limited access to healthcare and preventive services, food insecurity that leads to calorie-prioritizing food choices over nutritional quality, and chronic stress that disrupts sleep and hormonal balance. Children in low- and middle-income countries are particularly vulnerable, exposed to inadequate nutrition in early life while simultaneously facing high-fat, high-sugar, energy-dense foods that are lower in cost but also lower in nutrient quality — dietary patterns that, combined with lower levels of physical activity, result in sharp increases in childhood obesity. WHO This isn’t a personal failure — it’s a systemic one. Addressing childhood obesity without addressing poverty, inequality, and food system design is like mopping the floor with the tap still running.

Health Consequences of Childhood Obesity
So what actually happens to a child’s body and mind when they live with obesity? The consequences are wide-ranging, serious, and — if left unaddressed — lasting. This is not about aesthetics or social pressure. This is about real, measurable damage to developing bodies and minds.
Physical Health Complications
Compared to children with healthy weight, children with obesity are at a higher risk for asthma, sleep apnea, bone and joint problems, type 2 diabetes, high blood pressure, and mental health concerns like depression and anxiety. CDC These are conditions that were once considered adult problems, and seeing them manifest in children as young as six or seven years old represents a paradigm shift in pediatric medicine. Type 2 diabetes in children is particularly alarming — it’s a disease that can silently damage the kidneys, nerves, and cardiovascular system for decades, and the earlier it develops, the more cumulative damage it can cause over a lifetime. Sleep apnea in children affects cognitive development, academic performance, and behavior; children with untreated sleep apnea often appear inattentive or hyperactive, leading to misdiagnosis and inappropriate interventions. The cardiovascular risks are equally serious — high blood pressure, elevated LDL cholesterol, and early atherosclerotic changes have all been documented in children with obesity, laying the groundwork for heart disease decades before it would otherwise appear.
Mental Health and Emotional Impact
The psychological toll of childhood obesity is severe and often invisible. Children with obesity frequently experience bullying, social exclusion, and stigmatization from peers — and sometimes, painfully, from adults and even healthcare providers. This social cruelty isn’t just emotionally painful in the moment; it has measurable long-term effects on self-esteem, body image, academic performance, and mental health. Childhood obesity leads to extensive repercussions, elevating the risk of chronic conditions including not only physical diseases like diabetes and cardiovascular disease but also mental health challenges. Children dealing with obesity often face social stigmatization, diminished self-esteem, and academic struggles. PubMed Central Depression and anxiety are significantly more prevalent in children with obesity, and these mental health conditions can themselves perpetuate the cycle — emotional eating, reduced motivation for physical activity, disrupted sleep, and social withdrawal all contribute to further weight gain. Weight stigma doesn’t help children lose weight; it makes the situation worse and drives a harmful cycle of shame and avoidance.
The Long-Term Risks: What Happens When Obese Children Grow Up?
One of the most critical and sobering aspects of childhood obesity is its persistence. This isn’t something most kids simply “grow out of.” Research consistently shows that children with obesity are far more likely to become adults with obesity, and the health consequences compound with every passing decade. Childhood obesity is associated with a three-fold increased risk of mortality in early adulthood, and without intervention, the World Obesity Federation predicts the number of school-aged children and adolescents with obesity will rise from 150 million worldwide to over 250 million by 2030. SingleCare The economic dimensions are equally staggering. Annual direct healthcare costs attributable to childhood obesity in the United States in 2010 exceeded $14 billion, a figure expected to reach $45 billion by 2050. SingleCare The costs extend beyond direct medical care — lost productivity, school absenteeism, premature mortality, increased insurance premiums, and disability payments all add up to an enormous societal burden. At the global level, by 2035, the economic impact of overweight and obesity is projected to surpass $4 trillion annually. UNICEF These are not abstract projections; they are fiscal realities that governments and health systems are already beginning to confront.
| Health Risk | Increased Risk in Children with Obesity |
|---|---|
| Type 2 Diabetes | High — condition now appearing in childhood |
| Cardiovascular Disease | Elevated cholesterol, early hypertension |
| Sleep Apnea | Common; impacts cognitive development |
| Depression/Anxiety | Significantly elevated prevalence |
| Adult Obesity | Strongly predictive; high likelihood of persistence |
| Early Mortality | 3x increased risk in early adulthood |
How to Prevent Childhood Obesity
Prevention is always more effective — and less costly — than treatment. The good news is that childhood obesity is largely preventable, though doing so requires effort at multiple levels simultaneously. Think of prevention as a web, not a single thread — it requires schools, families, communities, governments, and the food industry to each pull their weight.
The Role of Parents and Families
Parents can help prevent childhood obesity by focusing on their child’s diet, activity, and sleep within the home through the teenage years, teaching kids healthy habits by modeling these behaviors themselves. NIH News in Health This is easier said than done in a world of tight schedules and food marketing, but the family home remains the most powerful environment for shaping long-term habits. Adopting healthy eating patterns as a family can help children grow healthfully and maintain a healthy weight as they age. Offering a variety of fruits and vegetables throughout the day, including frozen and canned options which are often less expensive than fresh, supports children’s nutritional health. CDC Beyond food, sleep is critically important and often overlooked. Getting enough sleep improves attention, behavior, and can help prevent type 2 diabetes, obesity, and injuries. Preschoolers need 10–13 hours of sleep per day including naps, children aged 6–12 need 9–12 hours of uninterrupted sleep a night, and youth aged 13–17 need 8–10 hours. CDC Reducing screen time is another high-leverage intervention that doesn’t require financial resources — it simply requires consistent boundaries and the willingness to replace screen time with family activities that involve movement.
Schools and Community Programs
Schools are arguably the most powerful institutional levers for childhood obesity prevention, because they reach virtually every child and can shape habits over a cumulative period of years. School nutrition programs that reduce access to junk food and increase the availability of whole foods, physical education requirements that provide daily movement, and health literacy curricula that teach children about nutrition and body autonomy all represent proven approaches. Finland has successfully reduced childhood obesity rates through a comprehensive approach that includes school-based interventions, community programs, and national policies. The “Schools on the Move” program encourages physical activity during school hours, while public health campaigns promote healthy eating habits. PubMed Central Community-level interventions — such as building safe parks, supporting farmers’ markets in food deserts, and creating after-school activity programs — extend the reach of prevention beyond school walls and into the environments where children actually live.
Treatment Options for Childhood Obesity
For children who already have obesity, prevention messaging alone isn’t enough. They need structured, compassionate, evidence-based treatment. And the treatment landscape has evolved significantly in recent years, moving well beyond “just eat less and move more.”
Intensive Health Behavior and Lifestyle Treatment (IHBLT)
In 2023, the American Academy of Pediatrics (AAP) published its first Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents with Obesity, establishing that a healthy lifestyle including good nutrition, optimal sleep, and physical activity continues to be the foundation of pediatric obesity prevention and treatment. NCCOR The gold standard intervention is known as Intensive Health Behavior and Lifestyle Treatment (IHBLT). This treatment happens face-to-face, engages the whole family, and involves at least 26 hours of nutrition, physical activity, and behavior change lessons delivered over three to 12 months. Cleveland Clinic The whole-family component is crucial — children don’t exist in isolation, and changing a child’s habits while leaving the rest of the family’s environment unchanged is a recipe for failure. IHBLT programs have shown real results, including improvements in BMI, metabolic markers, and mental health outcomes. Research from 2025 demonstrated that good response to pediatric obesity treatment was associated with reduced long-term morbidity such as type 2 diabetes, dyslipidemia, and hypertension, as well as lower incidences of mortality in young adulthood. NCCOR
Medical and Pharmacological Approaches
For children with severe obesity or significant obesity-related complications, lifestyle intervention alone may be insufficient. The medical toolkit for pediatric obesity has expanded in recent years. Certain medications have received FDA approval for adolescents, and bariatric surgery is considered in carefully selected adolescent cases. In December 2025, WHO published new guidelines on the use of GLP-1 receptor agonist therapies for the treatment of obesity, representing a significant pharmacological development in the field. WHO While these guidelines currently focus on adults, research into GLP-1 therapies for adolescents with obesity is ongoing and represents an important frontier. It’s essential to emphasize, however, that pharmacological treatment is never a replacement for behavioral and lifestyle change — it’s a supplement for specific clinical situations, used within a broader program of care. The goal is always long-term health, not simply a lower number on the scale. Any medical treatment must be accompanied by psychological support, nutritional education, and family engagement to have a lasting impact.

Conclusion
Childhood obesity is one of the defining public health challenges of the 21st century. It is complex, deeply rooted in social and economic inequality, driven by food environments that profit from children’s vulnerability, and devastating in its long-term consequences. But it is also largely preventable and treatable — and that is where our energy must be directed. Protecting the health of children means changing the systems around them: how food is marketed, what schools serve, what neighborhoods look like, and what support families receive. Individual action matters enormously, but it must be matched by structural change. Every child deserves to grow up in a world that makes the healthy choice the easy choice — and making that world a reality starts with understanding the full scope of the problem.
Frequently Asked Questions (FAQs)
1. At what age does childhood obesity typically begin to develop?
Childhood obesity can begin as early as toddlerhood, with evidence showing that weight gain patterns in the first two years of life can predict obesity risk later in childhood. Research shows that rapid weight gain during infancy is a notable early risk factor. Obesity rates tend to increase with age, with adolescents aged 12–19 showing the highest prevalence in U.S. data.
2. Can childhood obesity be reversed without medication?
Yes, in many cases it can. The cornerstone of treatment remains intensive lifestyle and behavioral intervention involving the whole family — including dietary changes, increased physical activity, reduced screen time, and improved sleep. For many children, especially when obesity is caught early, these approaches alone can produce meaningful and lasting improvements. Medication is typically reserved for severe cases or those with significant health complications.
3. How does socioeconomic status affect childhood obesity risk?
The correlation is well-established and strong. Children from lower-income families face higher obesity rates due to structural barriers including limited access to fresh, nutritious food; unsafe neighborhoods that restrict physical activity; fewer resources for sports and extracurricular programs; and higher stress levels within households. Poverty creates an environment where healthy living is genuinely more difficult, not simply a matter of personal choice.
4. Is childhood obesity linked to mental health problems?
Absolutely and significantly. Children with obesity are at substantially elevated risk for depression, anxiety, low self-esteem, and social isolation — in large part due to peer bullying and weight stigma. These mental health consequences can themselves perpetuate the cycle of obesity by reducing motivation for physical activity and increasing emotional eating. Comprehensive treatment programs must address mental health alongside physical health.
5. What role do schools play in preventing childhood obesity?
Schools are among the most impactful institutions for childhood obesity prevention. They influence what children eat at lunch, how much physical activity they get during the school day, and how much health literacy they develop. Evidence-based programs that improve school food quality, mandate daily physical education, limit access to sugar-sweetened beverages, and integrate health education into the curriculum have all demonstrated positive outcomes in reducing childhood obesity rates.